Neuro Diseases
- Aneurysms
- Arteriovenous Malformation
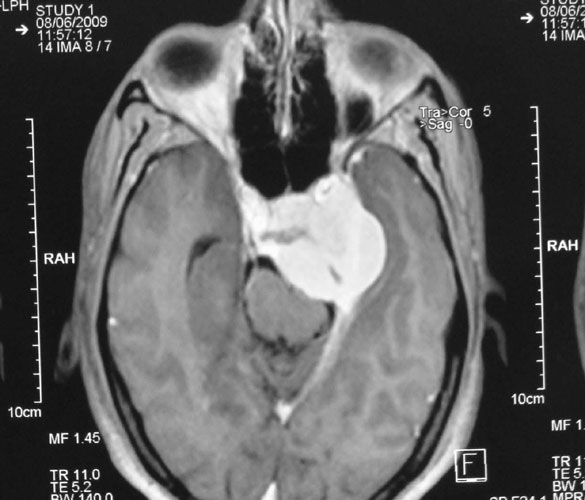
- Pituitary Tumours
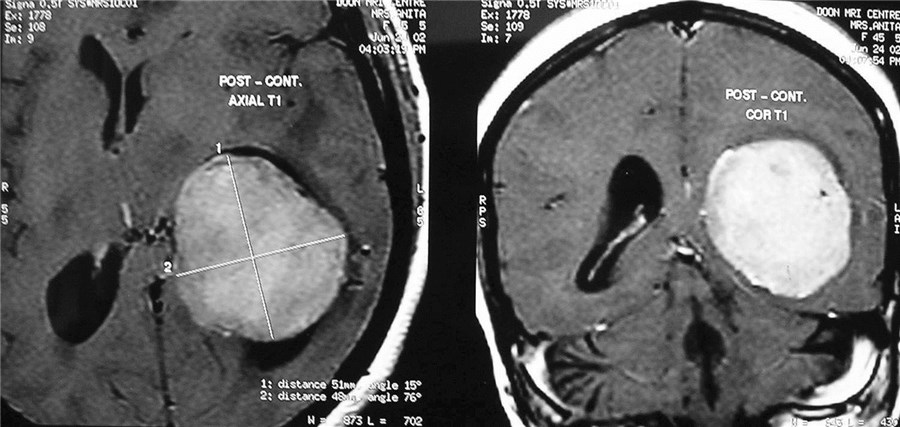
- Intracranial Meningiomas
- Keyhole Surgery
- Hydrocephalus
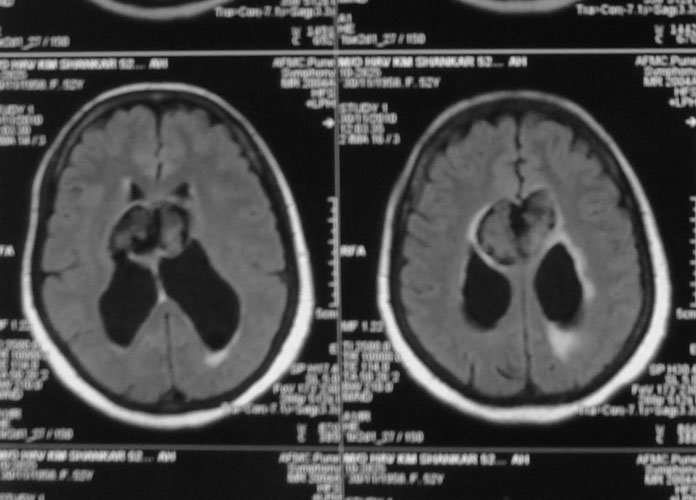
- Epidermoid
- Cervical Disc Disease
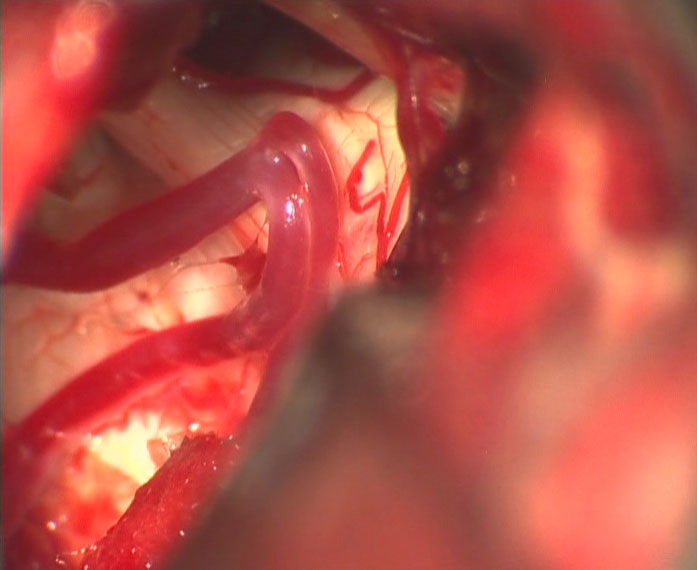
- Trigeminal Neuralgia
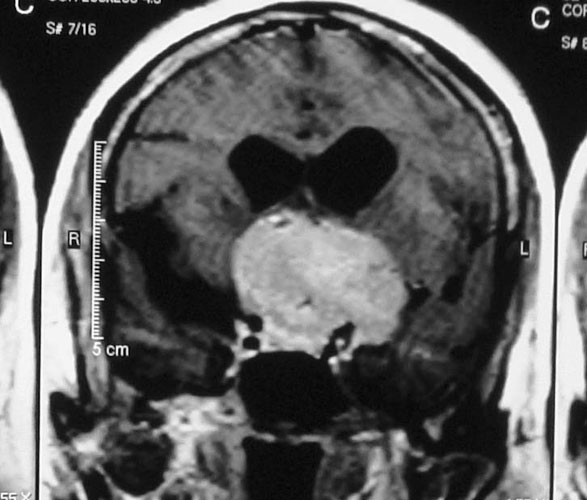
- Skull Base Meningiomas
- Intraventricular Meningiomas
- Gliomas
- Medulloblastomas
- Craniopharyngioma
- Encephaloceles
- Meningomyeloceles
- Hemifacial Spasm
- Ependymomas
- Pediatric Tumors
Aneurysms are balloon-like outpouchings from an intracranial artery, that can rupture and present as subarachnoid hemorrhage. SAH constitutes an emergency, and if severe can be life threatening. Management is early diagnosis by brain imaging and cerebral angiography, followed by definitive treatment in the form of surgical clipping or endovascular coiling.

Arteriovenous malformations of the brain are abnormal bunch of blood vessels that can rupture causing bleeding, or may cause seizures. Brain imaging (CT, MRI) is required for early diagnosis, while definitive treatment is carried out after cerebral angiography. Treatment implies craniotomy and excision of the AVM, which can be done safely in majority of the cases. Embolisation and radiosurgery are acceptable substitutes, but carry risk of further bleeding.





Pituitary is a small gland in the midline of skull base that has important role in maintaining hormonal milieu of the body. Tumors arising from pituitary present as gradually worsening partial blindness (‘field defects’), headache and endocrine abnormalities, commonest being acromegaly. Management involves a teamwork, with close association of neurosurgeon, endocrinologist and radiation oncologist. Surgery (through the nose or transcranial) is required to excise the tumor, followed by radiotherapy and management of hormonal deficiencies
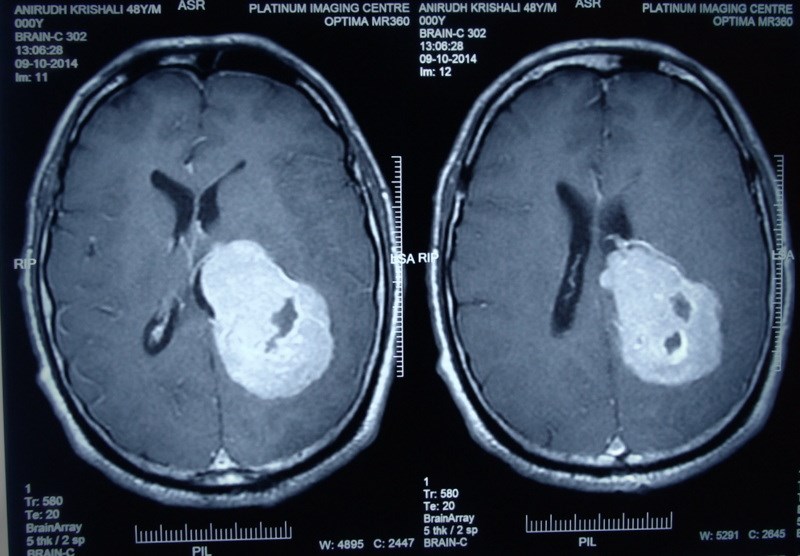
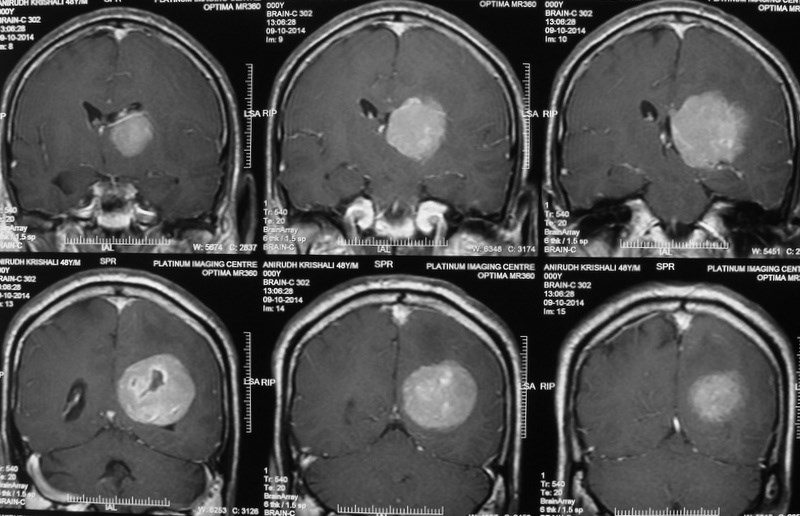
Meningiomas are solid, nodular (rarely, cystic), benign tumors that arise from the coverings of the brain, and compress the adjacent brain tissue. Usually present with headache, visual disturbances or weakness of half of the body. Diagnosis is by progression, especially if the tumor removal has been incomplete. Diagnosis is by MRI and surgery is curative.
Several pathologies in the brain can now be treated by small, precisely placed openings, aptly termed as ‘keyhole craniotomy’ The incision is small, made over the eyebrow, and a number of conditions can be treated by this small minimally invasive approach. These include tumors, aneurysms, epidermoids, etc. The results are extremely gratifying and the patients can be discharged early. The scar is practically invisible.








Hydrocephalus is a common problem in the childhood, due to obstruction to the flow of cerebrospinal fluid (‘clear fluid within the brain cavities’). Child presents with an enlarging head, headache, vomiting, drop in school performance. MRI is required to diagnose hydrocephalus, and to ensure that there is no brain tumor causing obstruction. Treatment is insertion of ventriculoperitoneal shunt from brain to the abdomen. In older children, endoscopic third ventriculostomy too can be considered.
Epidermoid is a cell rest in the nervous tissue which forms a cyst filled with keratin. It can occur in the brain or spinal cord. MRI gives accurate preoperative diagnosis. Surgery is safe and curative.






Cervical spine is the site of disc related problem that can present with neck pain, arm pain (‘brachialgia’). In severe cases, there may be compression of the spinal cord and weakness of both arms and legs. The diagnosis is made with MRI, and surgical treatment provides rapid relief. Surgery can be in the form of disc removal and insertion of a spacer, or insertion of an artificial disc.
The condition over one side of the face or jaw, often precipitated by eating, brushing teeth or touching. The underlying cause is an internal conflict between an abnormally placed artery and the trigeminal nerve (nerve that carries sensations from the face). While drug treatment and local injections can provide partial, short-term relief, surgery by microvascular decompression (separation of the offending artery from the trigeminal never) is the most effective and safe modality of treatment, which has the best results. Patient remains pain-free and drug free after surgery.

Meningiomas that arise from the base of skull need special planning for their safe and complete excision.









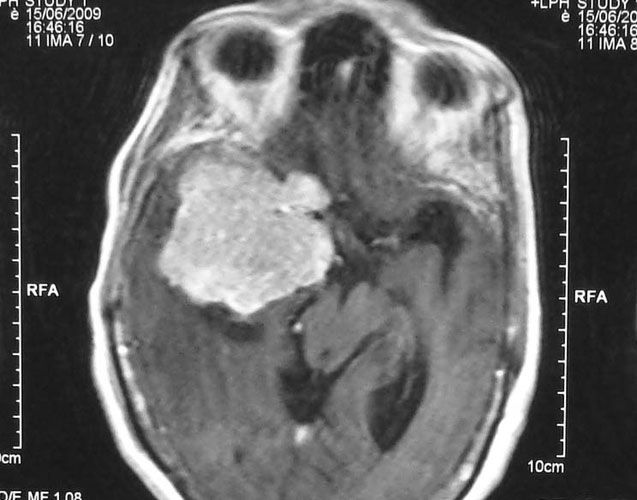


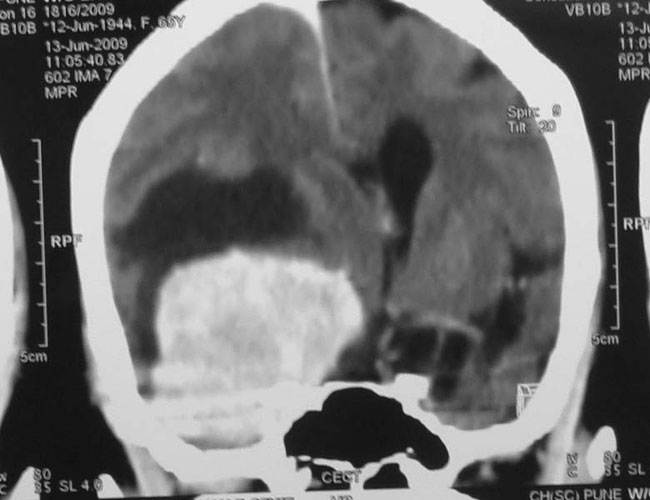



Meningiomas that occur within the ventricular cavities of the brain constitute a special group, and need special surgical planning to safeguard the vital areas of the brain.



Gliomas are brain tumors that arise from the supporting cells of the brain (‘glia’). These can be diffuse, involving large area of the brain or may be localized. They can be low grade (benign behavior), or high grade (malignant). They often present with headache, neurological weakness, etc and require early surgery for diagnosis, reduction of tumor mass, often followed by radiotherapy and chemotherapy.
Medulloblastomas are common tumors in childhood, often presenting with vomiting and headache. These tumors are located in midline of the cerebellum (back of the head). Diagnosis is made with MRI, and complete excision can be done safely in majority of the children.
Craniopharyngioma is a common tumor in childhood, but can also be seen in adults. These tumors often present with endocrine problems, abnormalities of appetite, visual problems. MRI gives diagnosis and treatment involves surgery. Attempt must be made at complete excision, with safeguarding of vital hypothalamic functions. Radiation may be required after surgery to halt tumor followed by surgical excision, with excellent results.
Click here to know more about Craniopharyngioma

Encephaloceles are often grotesque-looking congenital swellings arising from the head or face, that may make childbirth difficult. Child often appears to have a swelling as large as the head. Most of these swellings can be surgically removed successfully.










Meningomyeloceles are fluid filled midline swellings visible in newborn children at birth. They may contain neural tissue, and may be associated with hydrocephalus and weakness or complete paralysis of lower limbs. Management involves surgical removal and rehabilitation for lower limb paralysis, which does not recover.



Hemifacial spasm implies intermittent or persistent abnormal contraction of one half of the face due to conflict between an abnormally placed artery and the facial nerve (nerve that moves muscles of one half of the face). While botox injections can give short-term relief, the effect lasts about three months. Surgery (microvascular decompression) gives permanent cure and freedom from spasms as well as from requirement of repeated botox injections. Surgery involves separation of the offending artery from the facial nerve and is performed by a small (‘keyhole’) incision behind the ear. Long-term results are excellent.